
Senator Lindsey Graham died on Saturday, July 11, at the age of 71. A preliminary finding from the medical examiner pointed to an aortic dissection — a tear in the wall of the aorta, the major artery that carries blood away from the heart. The final death certificate has not yet been issued. Much of the reporting described his death as “sudden,” which is often how aortic disease appears: quiet until the moment it tears or bursts.
What can go wrong in the aorta
The aorta is the largest artery in the body, extending from the heart through the chest and into the abdomen. Several serious conditions can affect it. They are connected, but they are not interchangeable, even though they are frequently lumped together.
An aneurysm is a bulge. It forms when a weakened section of the aortic wall gradually stretches outward like a balloon. This process can unfold over many years and often produces no warning signs, which is why aneurysms are commonly discovered incidentally during imaging for another issue. Doctors define an aneurysm by its size: the larger it becomes, the thinner and more vulnerable the vessel wall grows, increasing the risk that it will eventually give way.
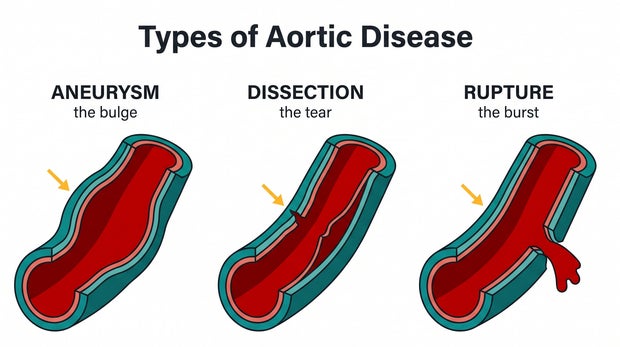
Illustration created with Gemini Nano Banana Pro / Dr. Céline Gounder
A dissection is a tear. Blood slips through the inner lining of the aorta and pushes into the wall itself, separating its layers and creating a false passageway. Unlike an aneurysm, this is typically abrupt and life-threatening, often causing sudden, severe chest or back pain described as ripping or tearing. It does not have to begin with an enlarged aorta. A dissection can occur in an aorta that never looked widened, one reason the diagnosis can be missed.
A rupture is a burst. The aortic wall fails completely, allowing blood to surge into places it should not be, such as the chest cavity or the sac surrounding the heart. It is the catastrophic outcome that can follow either an aneurysm or a dissection, and it is often fatal within minutes.
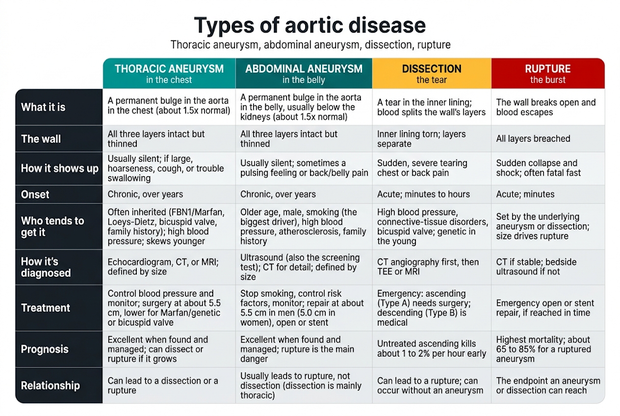
Table created with Gemini Nano Banana Pro / Dr. Céline Gounder
Bulge, tear, burst: the sequence can overlap, but the terms describe different events. A dissection is more common in older adults and is often linked to high blood pressure and arteries hardened over time. An aneurysm in a younger person, by contrast, more often raises concern for an inherited disorder affecting the body’s connective tissue.
That distinction is what separated Graham’s case from my husband’s. Graham, at 71, suffered a tear in an aortic wall shaped by years of what the medical examiner described as arteriosclerotic cardiovascular disease. My husband Grant Wahl had an aorta that bulged and then burst, at an age when this condition more often suggests an inherited vulnerability.
Graham’s type of aortic event is the more common one, associated with aging, hypertension and hardened arteries. For most people, it is not a signal to rush out looking for an aneurysm. It is a reminder to control blood pressure and for emergency departments to keep aortic tears in mind, because they can still be mistaken for heart attacks. In this area, there is one clearly established screening recommendation: a one-time ultrasound for men ages 65 to 75 who have ever smoked, aimed at detecting abdominal aortic aneurysms. Outside that group, very few readers need an immediate scan.
The version that killed my husband is the other one, and it doesn’t play by those rules. It runs in families, it strikes decades earlier, and it usually gives no warning until the artery fails. A routine checkup won’t find it, and no population screening program looks for it. Most families learn they carry it the way mine did, after someone dies. None of this is a reason for everyone to panic. But if aortic disease runs in your family, it can be caught early, with imaging and sometimes genetic testing, long before it turns dangerous.
The aneurysm nobody saw
In December 2022, my husband, the soccer journalist Grant Wahl, collapsed in the press box while covering a World Cup quarterfinal in Qatar. He died that night. He was 49.
The aneurysm was in the first stretch of aorta just above his heart, 6.0 cm across, and when it ruptured it filled the sac around his heart with blood. The autopsy found the wall had been thinning from the inside for a long time, its elastic fibers fragmenting. There was almost no hardening of his arteries at all. His was a bulge that burst in a man under 50, without the decades of arterial wear that killed the senator.
Why I asked for an autopsy
I’m a physician, epidemiologist, and medical journalist. I investigate. I think in terms of mechanisms and evidence, and I don’t accept “he died suddenly” as a stopping point. So I asked the New York City medical examiner for a full autopsy. I wanted to know what had happened, and I wanted an explanation. Had I missed something? Could anything have been done to prevent it or treat it? Could whatever killed him be used to protect the rest of Grant’s family, or help other families? I needed to make sense of it. Grief leaves you turning every ordinary day over, looking for the sign you didn’t catch, and the autopsy gave me answers instead of that loop. It gave me closure. It was therapeutic.
It gave me facts I needed for an uglier reason, too. Within days of Grant’s death, people invested in vaccine disinformation claimed the COVID shot had killed him. The autopsy was unambiguous: he tested negative for the virus, and the report stated that his prior vaccination “neither caused nor contributed” to the rupture. I’ve written about that elsewhere, and I’ll leave it there.
What the autopsy found in his DNA
The New York City medical examiner’s office runs the only molecular genetics laboratory housed inside a medical examiner’s office in the country. It tests the DNA of people who die suddenly, reviewing about 500 cases a year and finding a genetic cause in roughly 100 of them. In Grant’s heart tissue, the lab found a variant in FBN1, the gene behind Marfan syndrome.
Grant did not have Marfan. He was tall, but he didn’t have the syndrome. What he had was a single change in a gene that helps build the connective tissue holding the aortic wall together, in a spot the labs classify as a “variant of uncertain significance.” We don’t know for certain that this variant caused his aneurysm. It’s the most likely explanation, and inherited connective tissue problems are well-established risk factors for ascending aortic aneurysms in people under 60.
Sorting out which of these variants actually cause disease is real, unfinished work. Dr. Dianna Milewicz’s group at UTHealth Houston has spent years mapping the genes behind thoracic aortic disease. Other teams are chasing the opposite question: why some people carry a Marfan mutation and never get sick, hunting “modifier” genes that seem to shield the aorta. Grant’s variant sits inside that uncertainty.
Turning a death into prevention
None of that uncertainty changed what came next. Once the lab identified the variant, Grant’s blood relatives could be tested for that exact change. My brother-in-law Eric, Grant’s brother, carries it. His uncle, a niece and a nephew, and other family members have been tested, too. Eric had echocardiograms as well as MRI and CT scans. His aorta is structurally normal. He now gets regular imaging, and if his aorta ever starts to enlarge, his doctors will see it coming, with years to act.
That’s what the autopsy did. It gave the people who share Grant’s DNA something they could act on.
The same disease killed the actor John Ritter. In 2003, at 54, he died of an aortic dissection that was mistaken for a heart attack. His widow, Amy Yasbeck, started the John Ritter Foundation for Aortic Health, which funds Milewicz’s research program and has enrolled more than 1,500 families. Eric now advocates with them. Twenty-three years after Ritter’s death, aortic dissection is still routinely missed in emergency rooms because it mimics a heart attack and most clinicians aren’t thinking about it.
But it’s not just for patients to advocate for themselves. Clinicians should consider a tear in the aorta before sending someone home, and geneticists can test families after a sudden death. The New York City medical examiner recently launched a program called GIFTS that offers free genetic testing to the living relatives of people who died of inherited conditions, the first time a medical examiner’s office has tested living patients. The lab’s director, Dr. Yingying Tang, told me the program was shaped by families like mine.
Should you get checked?
Two questions I get asked a lot:
What should prompt you to get screened? A first-degree relative, a parent, sibling, or child, with a thoracic aortic aneurysm or dissection, or a sudden unexplained death in the family, especially before 60. Physical features of a connective tissue disorder: being very tall with long limbs, a chest that caves in or juts out, severe nearsightedness, or a dislocated lens. The current cardiology guidelines recommend imaging the aorta in the first-degree relatives of anyone with thoracic aortic disease.
One more, and it has nothing to do with family history: men 65 to 75 who have ever smoked should get a one-time abdominal ultrasound to check for an abdominal aortic aneurysm. If that’s you, ask your doctor for it.
Who should get genetic testing? People with a thoracic aortic aneurysm or dissection who also have features of a connective tissue disease, a family history of aortic disease, or disease before 60. When a disease-causing variant turns up, the rest of the family can be tested for that exact variant. That’s how you find the Eric’s, the ones carrying the risk whose aortas are still normal.
And if an aneurysm is found? A known aneurysm is a manageable condition: blood pressure control, regular imaging, and surgery once it reaches a size threshold, around 5.5 cm for the ascending aorta and lower for people with genetic forms. Grant’s was 6.0 cm, well into repair territory. Nobody knew it was there.
I couldn’t have known. He had no symptoms, and nothing in his life would have pointed a doctor to his aorta. But a lot of families can know. If aortic disease has touched your blood relatives, ask your doctor about imaging and ask whether genetic testing makes sense for you.
This article was originally published in Dr. Céline Gounder’s “Underlying Conditions” newsletter on Substack. Read more and subscribe here.















